
The ACSM Finally Updated the Resistance Training Guidelines: Why That Matters, What Changed, and Why Lifting Is Still One of the Most Important Things You Can Do for Your Health
For the past 15+ years, a huge amount of strength-training advice has been downstream from ACSM’s 2009 position stand, Progression Models in Resistance Training for Healthy Adults, with broader exercise guidance published in 2011. Those papers shaped how resistance training was taught in personal training certifications, exercise science curricula, physical therapy education, and general public health messaging. In many ways, they became the backbone of how people learned to talk about sets, reps, intensity, progression, and program design.
That older guidance was not “wrong,” but it was built from a dramatically smaller evidence base than we have now. The new 2026 ACSM position stand, Resistance Training Prescription for Muscle Function, Hypertrophy, and Physical Performance in Healthy Adults, is an overview of 137 systematic reviews including more than 30,000 participants. That is not a small tune-up. That is a major evidence upgrade. It gives us a much broader and more rigorous picture of how humans actually adapt to resistance training across different loads, frequencies, volumes, exercise types, and training styles.
One of the most important things about this update is not that it threw everything out and started over. It’s that clarified what matters most, what matters somewhat, and what the fitness industry has been dramatically overcomplicating for years. The old model helped popularize those neat little bins everyone can recite in their sleep: low reps for strength, moderate reps for hypertrophy, high reps for endurance. The new position stand does not say those categories are useless. It says the physiology is far more overlapping, flexible, and forgiving than the internet has been acting.
That flexibility matters, because one of the biggest barriers to lifting has always been the idea that you need the perfect program, perfect split, perfect exercise selection, perfect percentage, and perfect gym setup before you’re “doing it right.” The new paper pushes hard against that rigidity. It shows that resistance training improves strength, hypertrophy, and physical function across a range of setups, including circuit-based resistance training, elastic-band training, home-based resistance training, and more traditional gym-based lifting. In other words, the body is not nearly as precious and picky as social media likes to pretend.
What The 2026 ACSM Position Stand Recommends
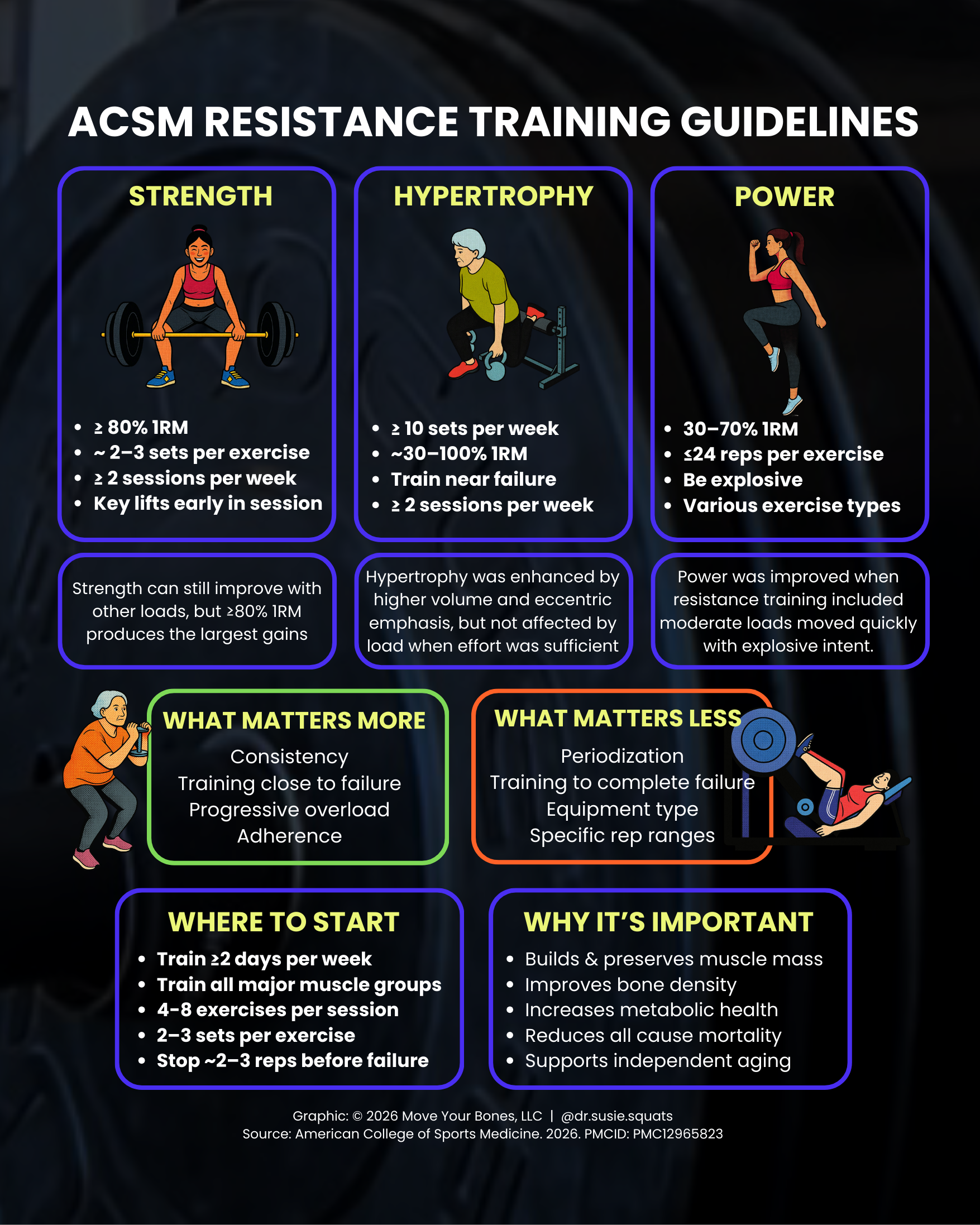
If the goal is strength, the variables associated with better strength outcomes were:
Load: at least ≥80% of 1RM
Frequency: at least ≥2 sessions per week
Volume: about 2–3 sets per session
Technique: full range of motion
Exercise order: key lifts performed earlier in the session
If the goal is hypertrophy, the variables associated with better muscle-growth outcomes were:
Volume: at least ≥10 sets per muscle group per week
Type: eccentric overload / eccentric emphasis
Load: hypertrophy occurred across a wide span of loads, from about 30% to 100% 1RM, provided effort was sufficient
If the goal is power, the variables associated with better power outcomes were:
Load: about 30%–70% 1RM
Volume: low-to-moderate total volume, roughly ≤24 repetitions × sets
Technique/type: Olympic-style weightlifting, power-focused resistance training, and a fast concentric phase
That is the tidy version. Here’s a COPYRIGHTED graphic I made for you. Now let’s get into the real meat cables.
Copyright 2026 Move Your Bones, LLC. Reproduction without permission is prohibited.
Why Strength Matters As Its Own Adaptation
Strength is your ability to produce force. That sounds obvious, but the implications are huge. Strength is not just a gym metric. It is a capacity reserve. The stronger you are, the bigger the gap between what life demands from you and what you are physically capable of doing. That reserve matters when you carry groceries, get off the floor, move furniture, pick up your kid, catch your dog, climb stairs, get out of a deep chair, or tolerate the repeated loads of running, hiking, sport, and daily life. Strength is also tightly tied to joint stability and tissue tolerance, because stronger muscles can absorb and generate more force, which changes how stress is distributed through the body.
That “buffer” idea is one of the most underappreciated reasons to lift. Pain, injury, and functional limitation often become more likely when life’s demands brush too close to your available capacity. Building strength raises that ceiling. It does not make you invincible, but it gives you margin. And margin is a beautiful thing. When daily life only requires a fraction of your available force-production capacity, movement feels easier, less threatening, and less exhausting. That is a huge quality-of-life win that has nothing to do with aesthetics.
Strength is also one of the most important predictors of physical function in older adults. Research consistently shows that declines in muscle strength are strongly linked to declines in physical performance and independence. In fact, evidence suggests muscle strength may influence physical performance even more than muscle mass alone. That distinction matters, because it is one reason why strength training should never be reduced to “just bodybuilding” or “just looking toned.” Force production is a functional trait. It is deeply tied to autonomy.
Why Hypertrophy Matters Beyond Aesthetics
Hypertrophy is the increase in muscle size, and it has been done so dirty by being framed as vanity-only for years. Yes, hypertrophy can change how you look. Shocking. Also true: muscle is metabolically active tissue that plays a central role in blood glucose regulation, insulin sensitivity, energy disposal, movement capacity, and resilience as we age. The new ACSM stand is very clear that hypertrophy is not trapped inside one magical rep range. Muscle growth can occur across a broad loading spectrum when effort is sufficient, and higher weekly volume appears especially important.
This is a very big deal because it widens the on-ramp. If someone cannot yet tolerate heavy loading, or only has access to dumbbells, resistance bands, machines, or bodyweight variations, that does not mean hypertrophy is off the table. It means programming can be adapted while still moving toward a meaningful muscle-building stimulus. That flexibility is one reason the 2026 update matters so much for public health and clinical practice. It makes resistance training more implementable, not less.
From a health standpoint, maintaining and building muscle is one of the clearest defenses we have against sarcopenia, the age-related loss of muscle mass and function. Sarcopenia is not just a cosmetic inconvenience. It is tied to reduced strength, slower gait speed, greater fall risk, lower functional capacity, and worse health outcomes over time. Resistance training is one of the most evidence-based strategies we have to preserve or increase muscle mass and strength as people age.
Muscle also matters metabolically. Meta-analyses show resistance training improves insulin sensitivity, including in older adults and in adults with overweight or obesity. The American Heart Association’s 2023 scientific statement likewise concluded that resistance training improves blood pressure, glycemia, lipid profiles, body composition, and broader cardiovascular risk factors. So when people act like lifting is optional but walking is the “real” health behavior, they are telling on themselves. Aerobic training matters. Resistance training also matters. Your pancreas, bones, connective tissue, and future self are not interested in the cardio-versus-lifting culture war.
There is also a mortality piece here that deserves more airtime. Systematic reviews and meta-analyses have found that muscle-strengthening activity is associated with lower risk of all-cause mortality and lower risk of several major chronic diseases, with some analyses estimating roughly 10%–17% lower risk and dose-response work suggesting the largest mortality benefit may occur at relatively modest weekly amounts. Resistance training is not merely for athletes or people chasing visible abs in fluorescent leggings. It is a health behavior with population-level relevance.
Why Power Deserves Way More Respect Than It Gets
Power is your ability to produce force quickly. It is not the same thing as strength, and this is where a lot of programs for general populations completely whiff it. You can be relatively strong and still be poor at expressing force rapidly. That matters because real life is not always slow and controlled like a textbook goblet squat demo. Real life is reactive. You trip on a curb. You catch yourself on the stairs. You need to step quickly to avoid falling. You reach, brace, decelerate, and redirect in fractions of a second. That is power territory.
Power is especially important in aging because it tends to decline earlier and more steeply than strength. That means someone can preserve a decent amount of force-producing capacity but still lose the speed at which they can access it. And that speed matters for fall prevention, gait, stair-climbing, chair rise performance, and broader physical function. Reviews in older adults suggest muscle power may actually be a more discriminating predictor of functional limitations than strength alone. That is a huge reason power training should not be treated like some niche performance-only add-on reserved for athletes doing box jumps in matching socks. It is part of aging well.
The ACSM update reflects that by highlighting moderate loads, lower volume, and intentional fast concentric intent for power development. This does not mean every person needs to be doing Olympic lifts from day one. It means that over time, a well-rounded program should include opportunities to move lighter-to-moderate loads with speed and intent, in a way that is appropriate to the person in front of you. Med ball throws, jump variations, rapid sit-to-stands, kettlebell swings, Olympic-lift derivatives, and speed-focused resistance exercises can all live somewhere on that spectrum depending on skill, health status, training age, and context.
One Of The Biggest Shifts: Hypertrophy Is Not Chained To 8–12 Reps
If there is one thing likely to cause gym-bro indigestion, it is this: the updated evidence does not support the idea that hypertrophy only happens in one narrow “muscle-building zone.” The 2026 position stand specifically notes that hypertrophy was not meaningfully changed by loads ranging from low to high when effort was sufficient. Other systematic reviews included in that evidence base have reported similar conclusions: low-load and high-load training can both build muscle, even if heavier loads are generally better for maximizing strength.
That does not mean load is irrelevant. It means load is one variable inside a bigger ecosystem that includes effort, volume, exercise selection, range of motion, and adherence. It also means a lot of people can stop acting like they have committed a felony if they get stuck with 15 reps on leg press one day. The body responds to tension, effort, and repeated exposure over time. It is less concerned with internet dogma than with whether you gave it a reason to adapt.
Training To Absolute Failure Is Not Required
Another important practical point from the new ACSM stand is that taking every set to absolute failure is not necessary for strength, hypertrophy, or power gains. The paper notes that sufficient effort can be achieved by training near failure, roughly around 2–3 repetitions in reserve. That is a very useful message for the general population, because many people swing between two extremes: training so easy that nothing meaningful happens, or training so hard, so often, that they hate lifting, flare symptoms, or fry themselves into inconsistency.
Near-failure training is the sweet spot for a lot of lifters because it preserves high effort without requiring psychotic all-out grinders on every set. It supports skill retention, fatigue management, recovery, and better long-term adherence. And adherence is the boring king of actual progress. The best program on earth does exactly nothing if you cannot sustain it.
[FREE GUIDE ON INTENSITY BASED TRAINING]
The Most Important Public-Health Problem Is Not Rep-Range Optimization
This is the part I think the fitness industry keeps missing while it argues with itself in circles.
Current U.S. surveillance data show that only about ONE in TEN adults meet guidelines for both aerobic and muscle-strengthening activity.
In 2024, Healthy People data estimated 26.4% of adults met both aerobic and muscle-strengthening guidelines during leisure time, while 32.9% met the muscle-strengthening target alone. Earlier CDC/NCHS data similarly found only 24.2% of adults met both in 2020, and 31.0% met the muscle-strengthening guideline with or without meeting the aerobic guideline. Among adults 65 and older, the numbers are even uglier; in 2022, only 13.9% met both guidelines, and Healthy People’s 2024 estimate for older adults was 15.5%.
So the biggest issue is not that people are doing 10 reps when they “should” be doing 8. It is not that they picked split squats instead of leg press. It is not that their hypertrophy block is not periodized by the moon cycle and the emotional state of their quadriceps. The real public-health issue is that most adults are not resistance training consistently at all.
And yes, I do think the real number may be worse than it looks, because these surveillance systems rely heavily on self-reported activity, which is subject to recall bias and social desirability bias. CDC materials specifically note those self-report limitations, and other research has shown self-reported physical activity often overestimates actual activity compared with objective measures. So when the numbers already look bleak, there is a decent chance reality is not prettier.
Why Lifting Is Non-Negotiable For Women In Particular
If there is one group that has been especially failed by mainstream fitness messaging, it is women. For decades, women were marketed movement as a shrinking project. Be smaller. Be lighter. Burn more calories. Do more cardio. Lift pink dumbbells if you must, but for the love of god do not accidentally acquire visible delts and a personality. That marketing had consequences. It steered women away from muscle-building and force-producing work during years when building and preserving muscle, bone, and connective-tissue capacity would have paid enormous dividends later. This part is social critique, yes, but it is also physiology.
Bone health is one major reason. Resistance training improves bone outcomes, and meta-analyses in postmenopausal women show dynamic resistance training and resistance-focused exercise can improve or help preserve bone mineral density, including at clinically important regions such as the lumbar spine, femoral neck, and total hip. Bone responds to mechanical loading. If you underload the skeleton for decades and then act surprised when osteopenia or osteoporosis shows up later, that is not your body betraying you; that is biology being consistent.
Muscle also becomes especially relevant across the menopause transition. Reviews note that declines in estrogen are associated with losses in muscle mass and function and may accelerate sarcopenic processes. Resistance training in postmenopausal women improves strength, body composition, physical fitness, and functional performance, and some evidence suggests that higher training volumes may be particularly important for maximizing hypertrophy in postmenopausal and older females. Put less politely: this is not the time to abandon lifting and hope a scented walking pad and three-pound dumbbells will hold the line.
There is also a quality-of-life piece here. The menopause transition can bring changes in body composition, insulin sensitivity, recovery, sleep, and perceived capacity. Muscle acts like a physiological reserve during that transition. More strength and muscle do not make someone immune to hormonal change, but they can improve resilience to it. That is why I view strength training for women not as a niche hobby and not as an aesthetic preference, but as preventative health care with a barbell, dumbbell, machine, band, or bodyweight attached to it.
Safety: Another Myth That Needs To Perish Tired
A lot of people still avoid resistance training because they think it is inherently dangerous, especially if they are older, deconditioned, dealing with pain, or coming back from time away. The new ACSM position stand explicitly addresses safety and notes that resistance training is safe for healthy adults of all ages. It cites large analyses showing exercise did not increase serious adverse events, and in data from adults with coronary heart disease, the nonfatal cardiovascular complications occurred during aerobic training rather than resistance training, while musculoskeletal issues during resistance training were linked to preexisting problems and resolved with modification. That does not mean lifting is risk-free, because nothing with a pulse is risk-free. It means the fearmongering around lifting has been wildly out of proportion to the evidence.
Done progressively and appropriately, resistance training is not reckless. It is one of the most adaptable things we can prescribe. Load can be scaled. Range of motion can be modified. tempo can be adjusted. exercise selection can change. support can be added. symptoms can be monitored. This is exactly why “I’m too old / stiff / weak / injured to lift” is usually the wrong conclusion. In many cases, those are the reasons you especially need a thoughtful entry point into resistance training.
What This Update Really Means In Practice
The headline change is not that ACSM discovered some magical new rep scheme from the heavens. The headline change is that the evidence base now supports a more nuanced, more flexible, and frankly more humane way to prescribe lifting. Strength still responds best to heavier loads. Hypertrophy is strongly influenced by enough weekly volume and sufficient effort, across a broad loading range. Power deserves specific attention because it underpins real-world function and falls off hard with aging. Near-failure is generally enough; full annihilation is optional and often dumb. And resistance training can be implemented in more ways than the old culture gave it credit for.
That matters for coaches, clinicians, and everyday humans because it shifts the question from “What is the one perfect way to lift?” to “What version of lifting can this person actually do consistently, progressively, and hard enough to adapt?” That is a much smarter question. It is also the one that gets more people training, which is the real point.
The Bottom Line
The new ACSM position stand is not exciting because it gave the internet new numbers to fight over. It is exciting because it better reflects reality. Human adaptation to resistance training is robust. It is flexible. It is responsive across a range of methods. And the difference between doing no lifting and doing some lifting is vastly more important than the difference between two otherwise reasonable programs.
If you care about bone density, metabolic health, muscle mass, joint capacity, fall resistance, independence, healthy aging, cardiovascular risk, and plain old feeling more physically capable in your life, resistance training is not a luxury. It is one of the most important health behaviors available to you. The tragedy is not that too many people are lifting “wrong.” The tragedy is that too many people have been convinced not to lift at all.
And for women especially, after decades of being told to stay small, light, and harmless? Building strength, muscle, and power is not just exercise. It is a long-overdue correction.
Start Lifting TODAY
If you’re reading this and thinking, “okay, I get it… but I still don’t know how to actually apply this,” I’ve got you! I created a free 4-week strength training program designed to help you actually meet these guidelines without overthinking it. It includes both home and gym options, breaks down common gym terms, and teaches you how to use intensity-based training so you can train close enough to failure to see results (without absolutely wrecking yourself). It also comes with an email series with all the “brain gains” I wish I had when I first started lifting, so you’re not just following a program, you actually understand what you’re doing and why.
[FREE 4 WEEK STRENGTH TRAINING PROGRAM]
And if you want more structure, guidance, and accountability beyond those first 4 weeks, that’s exactly why I created Supple Strength. It’s progressive, physical therapist-designed programming with multiple tracks (home and gym, 3- and 4-day splits), built to help you train for both today and the long term. Because this isn’t just about starting — it’s about staying consistent. The next block launches March 30th, and it’s designed to help you build strength, muscle, and resilience in a way that actually fits into your life.
Selected References
American College of Sports Medicine. Resistance Training Prescription for Muscle Function, Hypertrophy, and Physical Performance in Healthy Adults: An Overview of Reviews (2026).
American College of Sports Medicine. Progression Models in Resistance Training for Healthy Adults (2009).
CDC / NCHS physical activity surveillance and Healthy People activity targets for U.S. adults and older adults.
Paluch AE, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update (AHA scientific statement).
Momma H, et al. Systematic review and meta-analysis on muscle-strengthening activities and mortality/chronic disease risk.
Reid KF, Fielding RA. Review on skeletal muscle power as a determinant of physical function in older adults.
Shojaa M, et al.; Mohebbi R, et al.; Zhao F, et al. Meta-analyses on resistance training and bone mineral density in postmenopausal women.
Sá KMM, et al.; Thomas E, et al.; González-Gálvez N, et al. Reviews on resistance training in postmenopausal women, muscle mass, and function.